Triangular Interval & Quadrilateral Space Syndrome
Quadrilateral Space Syndrome

Quadrilateral space syndrome (QSS) happens when the axillary nerve is compressed, or injured in the back of the shoulder. Sometimes the symptoms are caused by the compression of an artery in the same area.
Quadrilateral space syndrome usually happens from overuse, especially with overhead sports like throwing and swimming. The syndrome can also be caused by an injury, like a shoulder dislocation.
Anatomy
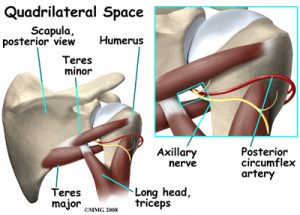
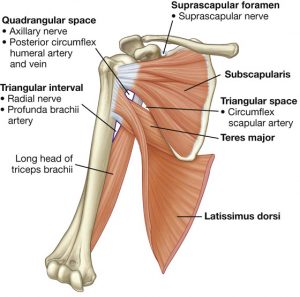
A quadrilateral is a four-sided shape. The quadrilateral space of the shoulder is in the upper back, where the shoulder meets the body. Three of the sides of the quadrilateral space are formed by muscles. The top of the quadrilateral is bordered by a muscle called the teres minor. The teres major muscle forms the bottom border. Part of the triceps muscle forms the inside border. The long bone of the upper arm, called the humerus, makes up the outer border.
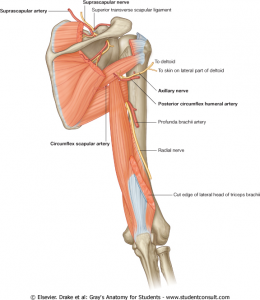
In addition to these muscles, the axillary nerve and the posterior circumflex humeral artery are in the quadrilateral space. When either the nerve or the artery is compressed or injured in this area it can cause problems such as quadrilateral space syndrome.

The axillary nerve is considered a peripheral nerve. There are several peripheral nerves in the shoulder that can be injured. The spinal cord in the neck, or cervical area, has branches that are called nerve roots. The nerve roots in the neck come together to form a large peripheral nerve called the brachial plexus. The axillary nerve is one of the branches off the brachial plexus. The axillary nerve is mainly formed from the fifth (C5) and sixth (C6) cervical nerve roots. The axillary nerve gives strength to the teres minor muscle and the deltoid muscle. It gives sensation to the shoulder joint.

The shoulder joint is also known as the glenohumeral joint. It is a ball and socket joint. The glenoid is the cup portion of the shoulder joint. The upper end of the humerus forms the ball portion.
The shoulder joint is supported by many muscles. The most famous are the four rotator cuff muscles.They combine at the shoulder to form a thick cuff. They are also referred to as the SITS muscles. Each letter stands for one

of the rotator cuff muscles; supraspinatus, infraspinatus, teres minor, and subscapularis. Sometimes injury to the quadrilateral space is mistaken as rotator cuff injury.
Causes
Repetitive stress or overuse is a major cause of quadrilateral space syndrome. Some of the more common causes of overuse are seen in overhead sports like throwing and swimming. Children specializing in certain sports at early ages, have increased risk of getting quadrilateral space syndrome. Sometimes poor training techniques are to blame. Bands of extra fibers are usually what cause the compression of the axillary nerve, or the small artery in the quadrilateral space.

There are varying degrees of nerve injury. Most commonly, injury to the axillary nerve is a more mild form of injury called neuropraxia. This means that it typically recovers fully. The axillary nerve is very short, so even a severe injury can heal rather quickly.

An acute axillary nerve injury can also happen from carrying a heavy backpack. The misuse of crutches can also cause compression of the nerve.
The most common traumatic injury that causes quadrilateral space syndrome (QSS) is a shoulder dislocation. Some reports show that quadrilateral space syndrome can happen 10 to 60 percent of the time after a shoulder dislocation. There is a greater risk depending on the type of dislocation.

A blunt force injury to the back of the shoulder can also cause quadrilateral space syndrome.
Symptoms
What does quadrilateral space syndrome feel like?

Symptoms of quadrilateral space syndrome usually include vague shoulder pain, numbness or tingling in the arm, and tenderness to pressure over the area of the quadrilateral space. A dull ache in the shoulder may worsen when the arm is moved overhead repeatedly.
Weakness and instability can sometimes be noted. The diagnosis of quadrilateral space syndrome is often missed since symptoms can be similar to other shoulder problems.
Diagnosis
Your doctor will complete a history and physical examination.
Your doctor will ask questions about activity, possible traumatic injury, and the symptoms you are having. The physical examination usually includes evaluating range of motion, strength testing, checking reflexes and sensation. During this examination pressure will be applied over various areas of the shoulder to see where it may be painful.
Weakness and instability can sometimes be noted. The diagnosis of quadrilateral space syndrome is often missed since symptoms can be similar to other shoulder problems. Often there will be wasting of the teres minor muscle, and sometimes the deltoid muscle. Subluxation (instability) of the glenohumeral joint is sometimes noted as well.
Your doctor may want you to have some special tests done in order to better evaluate what is causing your problems.
Nonsurgical Treatment
Most of the time, quadrilateral space syndrome will improve with nonsurgical treatment.
There are varying degrees of nerve injury. Most commonly, injury to the axillary nerve is a more mild form of an injury called neuropraxia. This means that it typically recovers fully. The axillary nerve is very short, so even a severe injury can heal rather quickly.
It is important to rest your shoulder. Your doctor may suggest taking a break from the activity that may be causing your symptoms. Changing throwing or sport mechanics may be helpful.
Anti-inflammatories (NSAIDs) such as ibuprofen or naprosyn may be suggested. Heat or cold packs to your shoulder may be beneficial.
Your doctor will likely prescribe physical therapy.
Triangular Interval Syndrome

Triangular Interval Syndrome (TIS) was described as a differential diagnosis for radicular pain in the upper extremity. It is a condition where the radial nerve is entrapped in the triangular interval resulting in upper extremity radicular pain. The radial nerve and profunda brachii pass through the triangular interval and are hence vulnerable.
The triangular interval has a potential for compromise secondary alterations in thickness of the teres major and triceps. It is described based on cadaveric studies that fibrous bands were commonly present between the teres major and triceps. When these bands were present, rotation of the shoulder caused a reduction in cross sectional area of the space. Normal resting postures of humeral adduction and internal rotation with scapular protraction may be speculated as a precedent for teres major contractures owing to the shortened position of this muscle in this position.
In addition, hypertrophy of this muscle can occur secondary to weight training and potentially compromise the triangular interval with resultant entrapment of the radial nerve. Shoulder dysfunctions have a potential for shortening and hypertrophy of the teres major. Shoulders that exhibit stiffness, secondary to capsular tightness, contribute to contracture and hypertrophy of the teres major. Hence, restricted external rotation can encourage adaptive shortening and thickening of the internal rotators of the shoulder principally the teres major and subscapularis. One may speculate that the lateral arm pain presented in shoulder dysfunctions may be of a nerve origin secondary to adverse neural tension of the radial nerve.

The triceps brachii has a potential to entrap the radial nerve in the triangular interval secondary to hypertrophy. The presence of a fibrous arch in the long head and lateral head further complicates the situation. Repeated forceful extension seen in weight training and sport involving punching may be a precedent to this scenario. The radial nerve is vulnerable as it passes through this space, for all of the reasons mentioned above.
Colgan Osteopathy in Kettering Northamptonshire
Colgan Osteopathy in Hatfield, Hertfordshire
To book an appointment, call 07738493974 or book online